
The shoulder is the most common cause of musculoskeletal disorders behind lower back and neck pain. ‘Rotator cuff’ is a term that many people may have heard when seeing a clinician in regards to shoulder pain – but would you be able to explain what it is?
Stability vs Mobility
When it comes to the design of the joints in our body, the two forces that are at conflict are stability vs mobility. We gain stability of a joint from the articular surfaces (this is how the bones fit together), the ligaments around the joint, and the muscular system that supports that joint. However as we increase the stability of a joint, often we have to trade the range of motion and degree of freedom that the joint has.
The shoulder and the hip joint are examples of ball & socket joints. However despite their similarities, you have a lot more freedom in regards to the shoulder and its mobility than you do with the hip. The shoulder joint trades the stability of a deep articular socket like that in the hip, to a shallower socket that allows more mobility. This shallow socket however means that the shoulder heavily relies on the surrounding muscles and ligaments for its stability throughout movement. These muscles that stabilise your shoulder joint are called your rotator cuff muscles.
Purpose of the rotator cuff
The rotator cuff consists of 4 muscles:
- Supraspinatus
- Infraspinatus
- Subscapularis
- Teres Minor
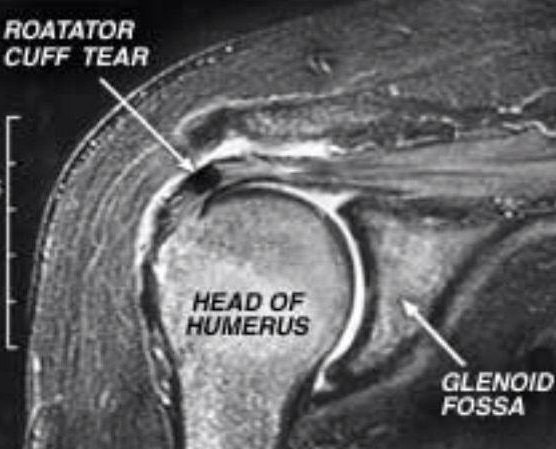
These muscles are very deep and close to the shoulder joint itself. They control the small adjustments to the position of the humeral head (ball component) inside the glenoid fossa (socket component) that allow proper movement. These aren’t considered the “main movers” when it comes to the shoulder, but they act to support and assist the larger muscles.
What can go wrong?
Rotator cuff injuries can occur throughout your lifetime. In younger individuals, the mechanism of injury is likely to be a fall on an out-stretched arm, getting the arm caught during a fall, or damage from overuse due to repeated overhead movements in sports i.e. volleyball, tennis, bowling etc. As we age, the incidence of these injuries increase, which is likely attributed to overuse or natural degeneration of the tissue through the aging process.
The incidence of rotator cuff tears increases from around 25 percent of individuals in their 60s, up to approximately 50 percent of those in their 80s.
It’s not unusual for individuals with rotator cuff-related issues to show no signs of pain or functional loss. However, completely asymptomatic individuals may develop symptoms in a short period of time.
How do we fix it?
Many patients will respond quite well to non-surgical interventions, with the help of a physiotherapist or exercise physiologist. Patients report significant relief in pain and improvements in function of the shoulder.
Conservative treatment will usually consist of:
Activity modification: This will involve finding your current functional capacity and slowly reintroducing daily activities as pain and strength allows. Complete rest is actually contraindicated for the recovery of rotator cuff injuries.
Strength exercises: A structured exercise program targeting your individual impairments will help restore movement and improve overall strength of your shoulder. An exercise program will include stretches and release work to improve mobility, and strength work to improve the muscles that support your shoulder to reduce pain and prevent further injury.
If the tear is substantial enough, or is completely torn, you may need to be referred on to a specialist for their opinion.
Exercises can be explained with more detail and tailored to your individual needs with the help of your treating physiotherapist.

References
Braun, C., Hanchard, N., Handoll, H., & Betthäuser, A. (2018). Predicting the outcome of conservative treatment with physiotherapy in adults with shoulder pain associated with partial-thickness rotator cuff tears – a prognostic model development study. BMC Musculoskeletal Disorders, 19(1). https://dx.doi.org/10.1186/s12891-018-2239-8
Edwards, P., Ebert, J., Joss, B., Bhabra, G., Ackland, T., & Wang, A. (2016). Exercise rehabilitation in the non-operative management of rotator cuff tears: A review of the literature. International journal of sports physical therapy, 11(2), 279–301.
Minagawa, H., Yamamoto, N., Abe, H., Fukuda, M., Seki, N., Kikuchi, K., Kijima, H., & Itoi, E. (2013). Prevalence of symptomatic and asymptomatic rotator cuff tears in the general population: From mass-screening in one village. Journal of Orthopaedics, 10(1), 8–12. https://doi.org/10.1016/j.jor.2013.01.008
Sambandam, S. N., Khanna, V., Gul, A., & Mounasamy, V. (2015). Rotator cuff tears: An evidence based approach. World journal of orthopedics, 6(11), 902–918. https://doi.org/10.5312/wjo.v6.i11.902
Sgroi, T. A., & Cilenti, M. (2018). Rotator cuff repair: post-operative rehabilitation concepts. Current reviews in musculoskeletal medicine, 11(1), 86–91. https://doi.org/10.1007/s12178-018-9462-7